

Vasectomy: Expectations and Effectiveness
What is it?
Vasectomy is a permanent form of male birth control. It is the most common, non-diagnostic procedure performed by urologists in the United States. Vasectomy is considered a reliable, effective, and low-risk procedure that can typically be done in the outpatient clinic setting in less than 30 minutes.
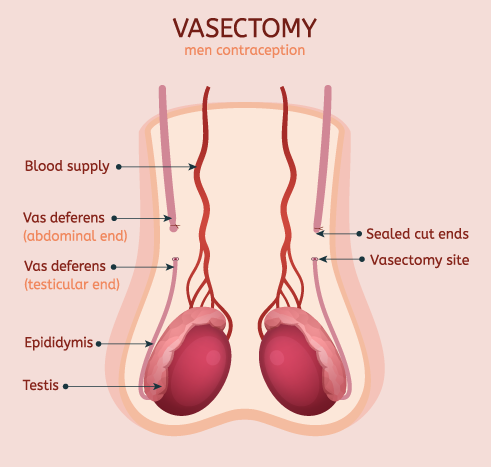
How does it Work?
Vasectomy works by eliminating sperm from your ejaculate. It is performed by blocking the tubes (vas deferens) that carry sperm from your testicles to your urethra and thus the outside world.
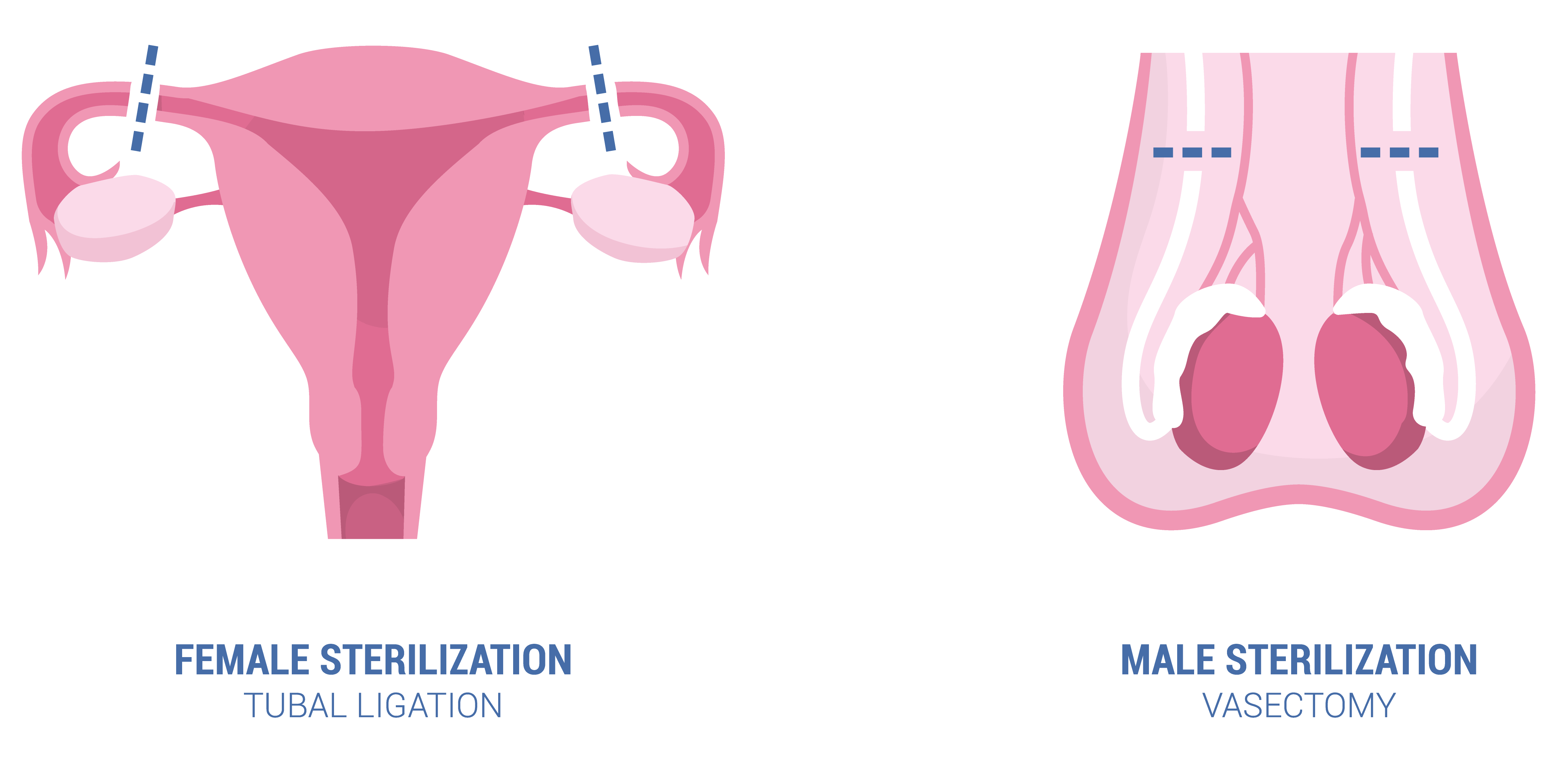
Vasectomy for Men or Tubal Ligation for Women?
If you and your partner are considering permanent contraception, you may have discussed vasectomy versus tubal ligation. I would urge couples to consider the following points:
-
- Vasectomy is one of the most effective contraceptives available – medical or surgical – and it is the most effective method for males
- Compared to tubal ligation, vasectomy is equally effective in preventing pregnancy; however vasectomy is considered a simpler, faster, and less expensive form of birth control
- Typically, vasectomy only requires local anesthesia (a numbing injection, no need for general anesthesia) and can be done in the urologist’s office, instead of the operating room
- The potential complications of vasectomy are considered less serious than those of tubal ligation, and generally men will have a quicker recovery time compared to female counterparts
- Vasectomy is typically about ¼ of the cost of tubal ligation, making it one of the most cost-effective of all methods of contraception
How is a Vasectomy done? The Approach
One of my urology mentors often used the phrase “There’s more than one way to skin a cat,” a mantra that is certainly true for vasectomy.
Let’s first tackle “minimally invasive” versus “no-scalpel.” To be clear, even a no-scalpel technique necessitates going through the scrotal skin. Rather than a small incision using a scalpel, the surgeon may use a sharp, pointed clamp to gently pierce and spread the skin apart, exposing the vas deferens beneath. Thus you’ll still need something to close the small opening(s) in your skin, such as skin glue, a Steri-Strip, or absorbable suture.
I prefer to use a single, midline incision in the scrotum approximately 1cm in length. From here I can access both the right and left vas. Some providers find it easier to make an incision on each side of the scrotum to access the vasa independently.
There are also multiple ways to achieve vassal occlusion (blockage of the vasa). Common techniques in the US utilize one or more of the following:
-
-
- Ligation/excision: occluding, cutting, and/or removing a piece of the vasa
- Mucosal cautery: burning of the vas ends
- Fascial interposition: securing a piece of tissue between two divided ends of the vas
- Titanium surgical clips or permanent sutures
-
I personally “clip, cut, and burn” – a triple insurance policy to guarantee we achieve our goal of sterility. In addition, I usually perform a fascial interposition, but certainly other combinations of the above can be just as effective.
Pain control: R.I.C.E. applies
Your urologist will utilize some form of numbing medication to keep you comfortable during your vasectomy. Some offices utilize oral anti-anxiety drugs or inhaled agents such as nitrous oxide, to keep the patient at ease during the procedure.
Post-operatively, patients usually do not need narcotic pain medications. Most of us are familiar with the Rest-Ice-Elevate-Compress pneumonic, and it should be used during your post-operative recovery. Common treatment regimens revolve around Tylenol® / Advil®, ice packs, and scrotal elevation and support.
Wearing tight-fitting underwear, such as athletic sliders or boxer briefs, will keep the testicles elevated the scrotum compressed. Similar to a sprained ankle, R.I.C.E will help reduce post-operative swelling and keep discomfort to a minimum.
Do I still need to use other contraception?
In the weeks following vasectomy – YES! Although no new sperm is reaching the outside world, it takes time for healthy, moving sperm to vacate the abdominal side of the vas deferens. The American Urological Association strongly advises that patients perform a post-vasectomy semen analysis (PVSA) to confirm sterility and provide assurances for the patient and his partner.
In my practice, I ask that the patient refrain from any sexual activity for one week post-operatively, and then ask him to engage in as much sex / masturbation as possible to “clean the pipes” – remember he still needs contraception during this time! I check a PVSA at 2-3 months and if negative, he is given the official title of “sterile.” Only then can the couple drop their other form of contraception.
Can it be reversed?
In short – yes, vasectomies can be reversed. However, I strongly urge all of my patients to consider vasectomy as a life-long decision. If there is any doubt regarding desire for future fertility, there are plenty of options available to prevent pregnancy while you reach a final decision. Remember, we are intentionally performing a procedure that is designed to achieve permanent sterility.
Regarding vasectomy reversals, it is important to note that most insurance companies do not cover this elective procedure. If the couple does not pursue vasectomy reversal, the only other option for that male to father a child is for sperm to be retrieved with a minor procedure, to be used with IVF/ISCI (in vitro fertilization / intracytoplasmic sperm injection) at a reproductive fertility center.
Vasectomy reversals require the skill of a specialist who is familiar with the microscopic reconstruction necessary for successful return of sperm to the ejaculate. So called “patency rates” have been linked to a handful of factors, including length of time since vasectomy, the patient’s medical history, and the skill of the surgeon. It is recommended that patients seek out a surgeon who has good experience with this procedure or who has undergone specialized training, in order to achieve the best outcomes.
Vasectomy myth busters
-
- Vasectomy will NOT lower your testosterone. Remember, vasectomy is not castration.
- Vasectomy will NOT increase your risk of prostate cancer. Mounting data has been compiled debunking this myth.
- Vasectomy will NOT affect your erections, urination, or ejaculation. This last one may surprise you, however the testes and epididymis only contribute about 5% of volume to the total ejaculate. So you’ll still reach climax like usual, and your ejaculation will be overall unchanged.
- Vasectomy will NOT decrease your sexual function. In fact, there are a small handful of studies that show erectile function can actually increases after vasectomy, as can sexual desire.
By the numbers…
-
- With proper technique, repeat vasectomy is necessary only in ≤1% of cases. 8 to 16 weeks after vasectomy is the appropriate time range for the first PVSA.
- The rates of surgical complications such as symptomatic hematoma and infection are 1-2%.
- Chronic scrotal pain associated with negative impact on quality of life occurs after vasectomy in about 1-2% of men. Few of these men require additional surgery.
Final thoughts
Most patients understandably have some trepidation regarding any procedure that involves such a private and sensitive area of their body. For those men who are secure in their family planning and looking for a permanent contraception solution, vasectomy is often the best option. I hope this article instills some confidence in the procedure, and provides discussion points for you to bring up with your urologist in an effort to create a treatment plan that is right for you.
Author:

Jonathan A. Beilan, MD
Fellowship trained urologist specializing in male fertility and sexual medicine
Advanced Urology Institute
430 Morton Plant St, Suite 206
Clearwater, FL 33756
Phone: (727) 441-1508
Website: AdvancedUrologyInstitute.com
Twitter: @JonBeilan