

Prostate Cancer Screening and Your Sexual Health
The prostate is the very first “P” in the PP&T of the Urologic Triad of Men’s Health, which are the common problems of the prostate, penis, and testicles men have as they journey through life. The primary functions of the prostate are reproductive in nature, as the gland provides 30% of the ejaculate fluid that mixes with fluid from the seminal vesicles and sperm from the testes to form the entire ejaculate volume.
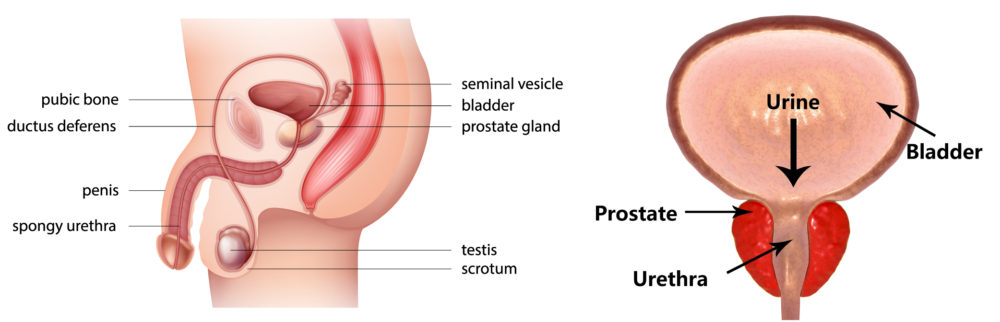
The prostate gland can cause a multitude of problems as men age. Common benign problems include enlarged prostate or BPH and infectious/inflammatory conditions such as prostatitis. An enlarged prostate can cause difficulty urinating due to the prostate’s location deep in the pelvis (pictured below). As you can see in the right portion of the picture the urethra (the tube men pee out of) runs right through the middle of the prostate. As men age the prostate continues to grow, while the bones of the pelvis limit the growth, which commonly results in an overgrowth of tissue that pinches the urethra tube closed. This results in a slow stream, frequency, and other urination symptoms. There are medical treatments, small office procedures (Rezum or Urolift), and surgeries (TURP, Greenlight, Simple Prostatectomy) that can treat these symptoms.
Another unfortunately common problem with the prostate as men get older is cancer. Prostate cancer is typically a disease of men 60 and older, however the trend seems to be younger patients being diagnosed. We have seen men as young as 40 being diagnosed, and even some patients in their late 40’s with advanced metastatic disease in our clinic. High-risk groups include men with a positive family history of prostate cancer and men with African American ancestry. Screening for cancer is one of the most effective ways we have to catch prostate cancer while it is localized in the gland and has not spread elsewhere. Screening consists of a blood test (PSA) and an experienced finger exam of the prostate to determine if there are abnormalities like firmness, nodules, or masses that would suggest cancer.
Screening is very important because prostate cancer usually does not cause any noticeable symptoms until it becomes locally advanced or spreads to other areas of the body.
The American Urological Association recommends screening for all men ages 55 to 70 with informed and shared decision making. For the high-risk patients screening should start at age 45. Screening should extend beyond 70 while the patient continues to be in good enough health to have a greater than 10-year life expectancy. Ultimately screening is very important because prostate cancer usually does not cause any noticeable symptoms until it becomes locally advanced or metastatic (spreads to other areas of body like the bones or pelvic lymph nodes) and because it allows us to detect and treat the cancer early. Screening is beneficial because we know 1 in 7 men will be diagnosed with prostate cancer and 1 in 40 will die from their disease. 30,000 men die each year due to prostate cancer. We do have effective treatments for these conditions including minimally invasive robotic surgery to remove the prostate and various forms of radiation. There are also many experimental treatments like HIFU, cryoablation, and focal therapy.
So, what does any of this have to do with your erections and ability to ejaculate? Well, as we said the prostate provides 30% of the ejaculate and it is an important part of the highway that carries semen out the end of the penis for the purposes of reproduction. Further, the nerves that control erections are on the outside portion of the prostate. What does this all mean? Well, if you have surgery to remove your prostate your vas deferens is usually cauterized and divided, and your prostate and seminal vesicles are removed. This means that highway for sperm to get into semen is blocked and the producers of 85% of the fluid of the ejaculate are gone. Further, sometimes when the disease is favorable (not outside the prostate and lower grade) we can spare the nerves on the outside by sweeping them away, but in the opposite situation where disease is advanced, the nerves are usually sacrificed to ensure removal of all the cancer.
Options for gentlemen with leaky veins in the penis as a result of prostate cancer treatment include high dose intracavernosal injection (ICI) therapy or outpatient surgery to place an inflatable penile implant.
Unfortunately, research shows that the 80/80 rule holds true regarding erections after a “nerve sparing” robotic radical prostatectomy. This means 80% of folks post-surgery will still not have erections hard enough for penetrative intercourse and 80% of the same group will fail medical erectile dysfunction therapy. The reason is men with ED as a result of pelvic surgery have leaky veins that prevent the blood from staying in the penis to cause erections. Remember, think of the penis as an inflatable rod. You need good blood flow and blood retention to create pressure and rigidity. If you have leaky veins it’s like having a hole in a tire. You can pump it up, but if there’s a leak, it isn’t going to stay up. Further, even if nerves are spared, common temporary paralysis can occur for up to 18 months. Leaky veins can be diagnosed with a doppler ultrasound of the penis. If you have leaky veins and want the ability to have penetrative intercourse, there are two treatment options: high dose intracavernosal injection therapy, or an outpatient surgery to place an inflatable penile implant (IPP). We recently published an article in the Journal of Sexual Medicine Reviews about patients who have had prior radical pelvic surgery (PRPS) and have IPP surgery that further explores these issues. Certainly, radiation to the prostate can have similar damaging effects, although they may be somewhat time delayed.
Penile rehab protocol for ED post prostate cancer treatment consists of PDE-5 oral medications and use of a vacuum erection device to promote blood flow and tissue elasticity.
We typically recommend a specific penile rehab protocol for ED after prostate cancer treatment starting at around 4-6 weeks as the patient heals. This consists of oral medications and a vacuum erection device (VED) to promote blood flow to the penis and stretching out the penile tissue. We prescribe daily, low-dose oral PDE-5 inhibitors such as 5 mg tadalafil lozenges (Cialis) or 20 mg sildenafil tablets (Viagra). We also ask patients to use a VED for 30 minutes a day WITHOUT the constrictive ring to stretch out the penile tissue and bring beneficial blood and nutrients into the penis. Patients with the best outcomes continue on PDE-5 inhibitors regardless if they produce an erection sufficient for intercourse. Some patients continue using PDE-5 medication even after penile implant surgery for the purposes of engorgement of the penile glans which the implant device doesn’t do. VED use is certainly important if the patient is no longer experiencing nocturnal erections because these are the typical benefits and presumed purpose of nocturnal erections. We also recommend max dose PDE-5 Inhibitors, 20mg tadalafil or 100mg sildenafil, twice weekly. If these interventions do not produce a satisfactory erection for intercourse, the doppler ultrasound of the penis combined with penile injection is the next step to further look at the blood flow to the penis. High dose penile injections can be used if oral medications do not produce satisfactory results, although some men may discontinue this treatment option due to the discomfort, inconvenient use, and a risk of scar tissue formation. If these interventions don’t produce satisfactory results or if they aren’t appealing to your lifestyle, then the Inflatable penile implant is an option that will provide satisfaction and up to 80% functionality 15 years post-surgery.
I hope you better understand just how important the prostate is in the Urologic Triad of Men’s Health. We’re here to help you deal with any and all problems men experience as they age and look forward to serving you, your family, and friends.
Author:

Jared J. Wallen MD
Urologic Surgeon and Men’s Sexual Health Specialist at Florida Hospital Physician Group
Office Locations in Brandon and Tampa, FL
Phone: (813) 278-8850
Website: mhurologytriad.org