

Peyronie’s Disease: Surgical Treatment Options
A diagnosis of Peyronie’s Disease (PD) can be difficult to deal with, but together we will navigate treatment options.
Think of the penis as an inflatable rod. It has two internal, side-by-side ‘cylinders’ called the corpora cavernosa positioned from the tip of the penis to the back portion of the pelvis. When a healthy man is aroused the cylinders fill with blood, the ‘rod’ inflates and becomes erect. As the arteries become engorged, the veins are compressed so blood is trapped in the penis and the penis remains erect. The penis typically regresses back to a flaccid state with lack of stimulation, sympathetic overdrive, or normal post ejaculatory physiology.

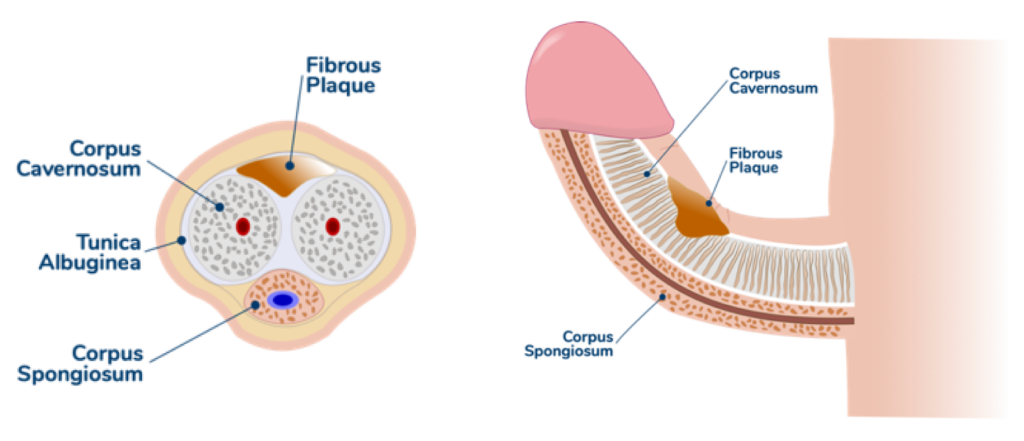
Around each cylinder is a very strong fascial layer like the fascia that keeps your abdominal contents inside you. This layer, called the tunica albuginea, is where PD occurs. During the erection process the scar tissue (plaque) associated with Peyronie’s prevents stretching and expansion in the area of plaque on the corpora causing a curvature, hourglass deformity, or another deformity when the penis is erect.
“Where the plaque occurs and in which layer it occurs determines the type of deformity”
The corpora have two layers; one is circular on the inside and the other is longitudinal on the outside. Where the plaque occurs and in which layer it occurs determines the type of deformity. Of note these severe deformities are found when the penis is fully erect and typically not in a flaccid state. However even in the flaccid state we are able to palpate (feel) areas of plaque, especially if it’s calcified.
PD is a scar tissue disorder that occurs in 10% of men and is more prevalent as men reach middle age. PD can also be a contributing factor to erectile dysfunction because the scar tissue can cause ‘venous leak ED.’ PD scarring may prevent the venous (blood vessel) valves from closing well enough to keep the blood in the penis from flowing back into the body’s circulatory system. The result of a venous leak is loss of the erection prior to the completion of sexual intercourse.
PD can certainly cause distress, physical and psychological pain, and impede a man’s ability to have intercourse or to participate in all forms of sexual activity.
The goal of any PD treatment is to achieve a ‘functional penis’ which means a penis as straight as possible with good erectile function. Obviously, if in the process of fixing your curvature and / or hourglass or other deformity we don’t want to harm your ability to have an erection.
Medical Treatments
There are many oral and injectable forms of medications that can help correct mild to moderate curvature or restore erection rigidity, however in more severe cases of curvature or if the patient has Peyronie’s and erectile dysfunction surgery can be indicated.
Surgical Options
There are 3 types of surgical procedures typically done for PD, alone or in combination:
-
- Penile plication
- Incision or excision of plaque and grafting
- Placement of penile prosthesis alone, with modeling, with internal incision of plaque (the ‘scratch’ technique), or with incision or excision of plaque and grafting
Penile Plication
During penile plication the surgeon uses sutures underneath skin on the opposite side of the curvature to create an opposing tension to correct the curvature. This surgery is most often done if the patients’ erectile function is good and oral or injectable PD treatments have failed to correct the deformity. The primary patient concern with this procedure is the risk of some loss of penile length as a result of plication surgery.
The rendering below illustrates the theory of plication. The blue dotted line represents sutures placed by the surgeon under the skin and into the corpus cavernosum on the opposite side of the maximum curvature. The red arrow represents the length of corpora tissue bunched together when the suture is tied down by the surgeon. Typically, the corpora spongiosum is lifted away from the corpora cavernoma’s surface first and not included in the sutures, and there would be smaller distance of corpora included in each stitch to limit the loss of length. This rendering has been simplified for ease of understanding.

The sequential bunching of tissue to counteract the plaque that’s causing curvature is what causes a risk of length loss. A more severe curvature requires more sutures and likely results in more penile length loss.
Incision or Excision of Plaque and Grafting
Incision or excision of plaque and grafting surgery requires more skill and is reserved for patients with severe deformity and / or erection issues. A ‘relaxing’ incision or incisions are made in the area of maximum curvature to ‘release’ the scar tissue deformity, or in more severe cases the scar tissue is removed in a larger section. After this is performed, a graft material is placed to ‘patch’ the area of the resulting gap or imperfection. The graft may be sewn in place or special self-adherent grafts can be used.
“…incision or excision of plaque and grafting surgery is commonly performed in combination with placement of an inflatable penile prosthesis”
The biggest risk with this type of surgery is if in the process of correcting the deformity by cutting and removing the plaque we impact erectile function, penile sensation, or alter other functions in the area. One way to describe how this procedure could cause ED is to compare it to patching a tire. Think of the corpora cavernosa as the rubber on the outside of the tire. If we cut out a section or make an incision in the rubber and apply an external patch to the area (which is not done to tires) it would be very hard to obtain a tight seal that will hold pressures as high as 50 psi in the case of the tire, or 120 mmHg for the corpora. Due to these possible outcomes, incision or excision of plaque and grafting surgery is commonly performed in combination with placement of an inflatable penile prosthesis.
Placement of Penile Prosthesis
Outpatient surgery to place either an inflatable or semi-rigid (bendable rod) penile implant may be indicated for patients with severe curvature, erectile dysfunction, or risks of surgical complications. These devices are permanent prosthetic implants that provide ‘on-demand’ erectile function by pumping up the inflatable type by hand through the skin of the scrotum, or bending the semi-rigid type into position.
Penile prosthetic devices are not visible after surgical placement and healing and can function up to 20 years without issue. This surgery requires patients to stop taking anticoagulation medications and have appropriate surgical clearance. The risks of implant surgery may include bleeding, infection (1-2% of patients during the healing process), and in rare cases erosion of the implant, device malfunction, need for revision surgery, pain, cosmetic dissatisfaction, perforation of the urethra, or severe bowel/bladder/vascular injuries.
It should be noted that the device provides erectile function, but the function is somewhat different than natural erections given that there is a prosthetic in place.

The inflatable devices tend to be more common as they offer both the erect and flaccid states of a natural penis. One important thing to understand is that a penis with implant in the flaccid state will look more ‘pronounced’ than a penis without an implant in the flaccid state because the device is taking up space even when not inflated.
“Placement of an implant should correct erectile dysfunction without changing the ability to ejaculate, achieve orgasm, or changing penile sensation”
Furthermore, with an inflatable prosthesis the transition between flaccid and erect states is operator dependent due to the manual pump. A semi-rigid device tends to be a better option for a man that is desiring erectile function but has poor manual dexterity. Placement of an implant should correct erectile dysfunction without changing the ability to ejaculate, achieve orgasm, or changing penile sensation. An Implanted Penile Prosthesis (IPP) can be used in the following settings for Peyronie’s:
Penile Prosthesis Placement Alone
If the curvature is less than 30 degrees and pre-op erectile function is poor, placing an IPP can be indicated for correction of curvature and maximum rigidity. Remember the goal is a mostly straight, rigid erection.
Penile Prosthesis Plus Modeling
In instances of more severe curvature the surgeon may combine placement of a penile prosthesis with specific ‘modeling’ maneuvers to stretch the penis in the opposite direction of curvature to help release the curve. These maneuvers are similar to stretching exercises patients are given during the treatment of PD with injection therapy and are done by the surgeon during the implant surgery. Sometimes patients are instructed by their surgeon to perform stretching exercises when fully healed from the implant surgery. In these cases the patient will inflate their device to create a rigid erection and preform the exercises to help further correct their curvature. This should only be done at the direction of your physician.
Penile Prosthesis Plus Internal Incision of Plaque
The ‘scratch technique,’ developed by Dr. Paul Perito, may be combined with the placement of a penile prosthesis. In this case, the surgeon will make small ‘scratches’ or incisions in the area of plaque to weaken the scar tissue and allow the prosthesis be more effective at straightening the penis. Because of the way this technique is performed, it is exclusively performed in combination with penile prosthesis surgery.
Penile Prosthesis Plus Incision or Excision of Plaque and Grafting
This technique is described above and often performed in combination with placement of a penile prosthesis to ensure post-surgery erectile function is satisfactory for sexual activity.
We sincerely hope that after reading this blog you have greatly increased your understanding of what options may be available from a surgical standpoint to treat your PD and correct your deformity while still maintaining or replacing your erectile function.
Author:

Jared J. Wallen MD
Urologic Surgeon and Men’s Sexual Health Specialist
YOU & WEE Urologic Surgery and Wellness
Tampa Bay Area, FL
Phone: (941) 212-1600
Website: www.youandwee.com